

Clivo-axial Angle (CXA)
Radiologists look for specific indicators of an abnormal craniocervical junction (i.e. where the neck attaches to the head) using specific measurements. One of the key indicators is an abnormal clivo-axial angle (CXA) measurement.
The clivo-axial angle (CXA) measures the alignment of a portion of the skull base and the second vertebrae (C2) of the upper cervical spine. It is one of the key radiology measurements used to assess and rule out craniocervical instability (CCI).
Abnormalities in this angle may indicate misalignment or instability, which may stretch the brainstem and spinal cord, obstruct cerebral spinal fluid (CSF) and blood flow, and cause neurological symptoms. A few studies have found that a smaller CXA was associated with more severe neurological symptoms and higher disability scores.

Basic Anatomy
The cervical spine is connected to the head in an upright position, and it needs to be tilted to allow fluid like cerebrospinal fluid (CSF) to flow up to the brain. This “tilt” is measured by the clivo-axial angle (CXA).
What is considered abnormal and normal CXA measurements in neutral position on imaging?
-
-
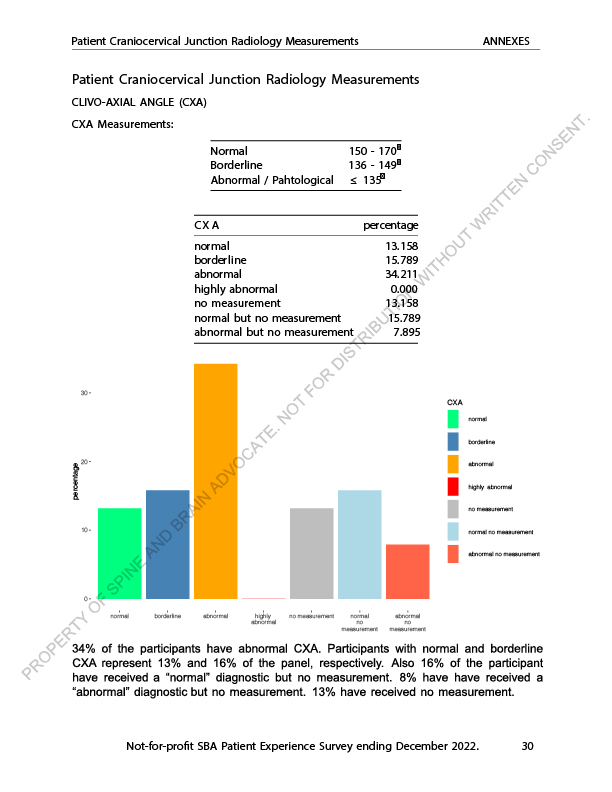
- Normal: 150° – 170°
- Mildly abnormal (borderline): 136° – 149°
- Abnormal: greater than 170° or equal to / less than 135°. An angle of 135° or less is considered potentially pathological.
-
What are the causes of abnormal CXA measurements?
Many conditions (congenital and acquired) cause abnormal CXA measurements. This includes Chiari malformations, osteogenesis imperfect, achandroplasia, Down’s syndrome, Ehlers Danlos Syndrome (EDS), inflammatory conditions like rheumatoid arthritis and lupus, trauma involving the neck region, and infections such as TB spondylitis.
What symptoms does an abnormal CXA measurement produce?
Common symptoms include reduced neck range of motion, neck pain, sleeplessness, feeling of faintness, pain around the ear, ringing in the ear, feeling of spinning, vision problems, paresthesia (numbness), and problems controlling urine and bowel movement.
What are some structural abnormalities are associated with abnormal CXA measurements?
Abnormal CXA measurements, for example a kyphotic CXA of 124° result in a mechanical deformity and lengthening of the brainstem and upper spinal cord. Reference
A kyphotic CXA of 120° is considered abnormal because it means that the cervical spine has become more curved which can result in compression of the brainstem, spinal cord, and other contents of foramen magnum. This can cause functional Chiari Malformations, and central and peripheral central nervous system stress.
6. What Type of Medical Imaging is Needed to Assess CXA?
Imaging of the cervical spine and craniocervical junction may be done while patients are lying down (supine imaging), or in a standing position (upright imaging) while moving the neck in different positions, which is called dynamic imaging.
Neurosurgeons and radiologists who specialize in craniocervical instability and abnormalities of the craniocervical junction rely on either supine or dynamic upright MRI, CT Scan or upright Cone Beam CT (CBCT) scans in neutral, flexion and extension positions to assess the neck in different positions as well as possibly (and preferably) in weight-bearing (upright) position, as an advanced method to assess the craniocervical junction. Although research on dynamic imaging is relatively new and small, and it is not widely understood at this time, more and more specialists are beginning to utilize upright dynamic imaging.
For dynamic imaging, Anoushesh and colleagues in a study reported a mean value for extension CXA as 169.20°, and 144.73° for flexion CXA. Reference
In another paper, a normal CXA is approximately 155°, decreasing 10° in flexion and increasing 10° in extension. Reference
Another study referenced flexion CXA normal range at 134° to 163° and extension CXA normal range at 152° to 179°.
When to Consult a Neurosurgeon?
If a patient’s radiology report states the CXA is abnormal / pathological, a consultation with a neurosurgeon is necessary, especially if neurological symptoms are present. Note that it is important to find a neurosurgeon who understands dynamic imaging, otherwise, they may be relying on traditional methods of assessing the craniocervical junction and may overlook key findings.
For a borderline CXA measurement, it does not automatically mean surgery is necessary unless there are additional signs of progressive instability or clinical symptoms requiring intervention, yet it is crucial for patients to consult with a neurosurgeon for a full assessment.
Excerpt from Craniocervical Junction Patient Experience Survey 2022 – Participant CXA Measurement Radiology Summary
Roughly over 36% of the survey participants did not receive a CXA measurement on their original radiology report. Over 1/3 of patients that received a CXA on their report, had an abnormal CXA measurement, indicating neurosurgical consultation would be helpful.
Abnormal CXA and Its Relation to Neurodegenerative Disorders
An abnormal CXA, such as a kyphotic CXA, can result in stretching of the nerve bundles that are contained within the brain stem and spinal cord leading to the collection of small proteins that make up the cell body (neurofilament) in the cable-like fibers (axons) that carries electrical signals between nerve cells, which cause cell death (apoptosis). This may lead to faulty craniospinal hydrodynamics increasing the chances of neurodegenerative disorders such as Alzheimer’s Disease, Parkinson’s Disease, Multiple Sclerosis, Obstructive Sleep Apnea, and others.
What Conservative and surgical treatments are available?
Conservative management includes physical therapy, cervical curve restoration therapy, upper cervical chiropractic, bone marrow concentrate or platelet rich plasma injections into ligaments and muscles that may help them to tighten or get stronger.
Neurosurgical interventions include craniocervical fusion (also called atlanto-occipital fusion etc.) .
Foramen magnum decompression (FMD) is the primary surgical treatment for symptomatic Chiari Malformation 1 (CM1).
Additional Information on Clivo-axial Angle (CXA)
The CXA radiology measurement of the craniocervical junction is recognized around the world and utilized in majority of continents. The following are a few articles that focus on CXA.
USA Article
“No major complications were observed. Two patients showed pedicle screws adjacent to but not deforming the vertebral artery on post-operative CT scan. All clinical metrics showed statistically significant improvement. Mean CXA was normalized from 135.8° to 163.7°. Correction of abnormal CXA correlated with statistically significant clinical improvement in this cohort of patients. The study supports the thesis that the CXA maybe an important metric for predicting the risk of brainstem and upper spinal cord deformation. Further study is feasible and warranted.” Reference
Canadian Article
“Based on our systematic review, we recommend that the CXA, Harris measurement (BDI & BAI), Grabb-Mapstone-Oakes measurement, and the angular displacement of C1 to C2 be used to evaluate suspected craniocervical instability (CCI) in EDS patients. Surgical fixation of suspected CCI should only be performed in cases with clear radiographic presence of instability and concordant symptoms/signs. Consensus-based guidelines and care pathways are required.” (Canada) Reference
Philippines Article
“There has been a drastic rise in patients with neurodegenerative and functional disorders in the past decade, and early detection of such conditions is not yet feasible. Upright posture and motion of cervical spine increase the strain in craniocervical junction (CCJ) which is a crucial tollgate for cerebrospinal fluid and blood flow between spinal canal and cranial vault that may lead to faulty hydrodynamics in the craniospinal region and furthering to edema, chronic ischemia, and hydrocephalus…
The clivoaxial angle (CXA) or upper cervical angle and cranial base angle, both are important for the function of the brainstem and cord. As classically described by Chamberlain, a lower than normal CXA (150–165°) compresses the brainstem, cord, contents of foramen magnum, and spinal canal . This not only causes functional Chiari formations but also predisposes the individual to biomechanical neuraxial stress which is manifested by myelopathy, bulbar symptoms, and neck pain or headache…
Biomechanics and mechano-biology are closely interrelated, neuronal bundles being the pathological substrate of deformative stress in this case due to kyphotic CXA directly leading to stretch triggered accumulation of neurofilament in axons and thus apoptosis. An abnormal CXA may lead to faulty cranio-spinal hydrodynamics increasing the chances of neurodegenerative disorders such as Alzheimer’s, Parkinson’s, multiple sclerosis, obstructive sleep apnea, etc….” (Philippines) Reference
Case Study Article by Austrian Trained Physician
A severe case of platybasia and basilar invagination. Platybasia can be caused by a wide variety of congenital and acquired diseases. Clivoaxial angle (CXA) = 83 degrees (cut-off value: 138.5 degrees). Reference
SBA Written by Dr. E. Deng 2023